NK and B cell Subset Assessment in Type I Diabetes Patients on Waitlist for Pancreas Transplantation
Shafaq R. Rizvi1, Ravinder Jeet Kaur1, Vikash Dadlani1, Yahya Almodallal2, Corey L. Reid1, Byron H. Smith3, Walter Kremers3, Aleksandra Kukla4, Mark D. Stegall5, Amir A. Sadighi Akha6, Yogish C. Kudva1.
1Division of Endocrinology, Diabetes, Metabolism, & Nutrition, Mayo Clinic, Rochester, MN, United States; 2Department of Medical Oncology, Mayo Clinic, Rochester, MN, United States; 3Department of Biomedical Statistics and Informatics, Mayo Clinic, Rochester, MN, United States; 4Department of Nephrology and Hypertension, Mayo Clinic, Rochester, MN, United States; 5Department of Surgery and Immunology, Mayo Clinic, Rochester, MN, United States; 6Department of Laboratory Medicine and Pathology, Mayo Clinic, Rochester, MN, United States
Introduction: Type 1 Diabetes (T1D) is an immune mediated disease with near complete destruction of beta cells. About 40 % patients with T1D develop End Stage Renal disease (ESRD) during their lifetime and require kidney and/or kidney pancreas transplantation. Recent genetic studies have described differences in genomic regions associated with immune responses and types of cells infiltrating islets between patients with early onset of diabetes (< 7 yrs.) and later onset of diabetes (≥ 7 yrs.). Limited data are available regarding immune profiles of these subsets of patients especially when evaluated for transplantation. Therefore, we studied flow cytometric profiles of immune subsets in these patients with the long-term vision of developing personalized immunosuppression.
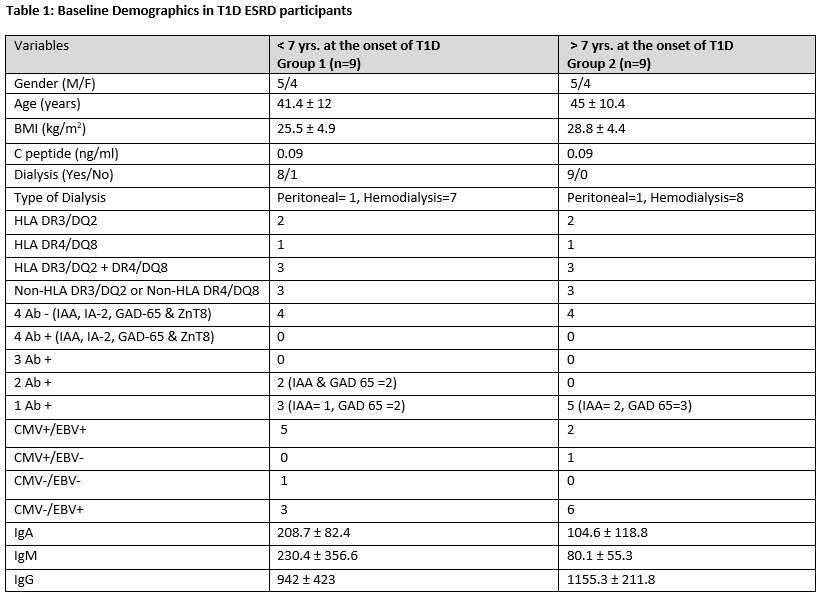
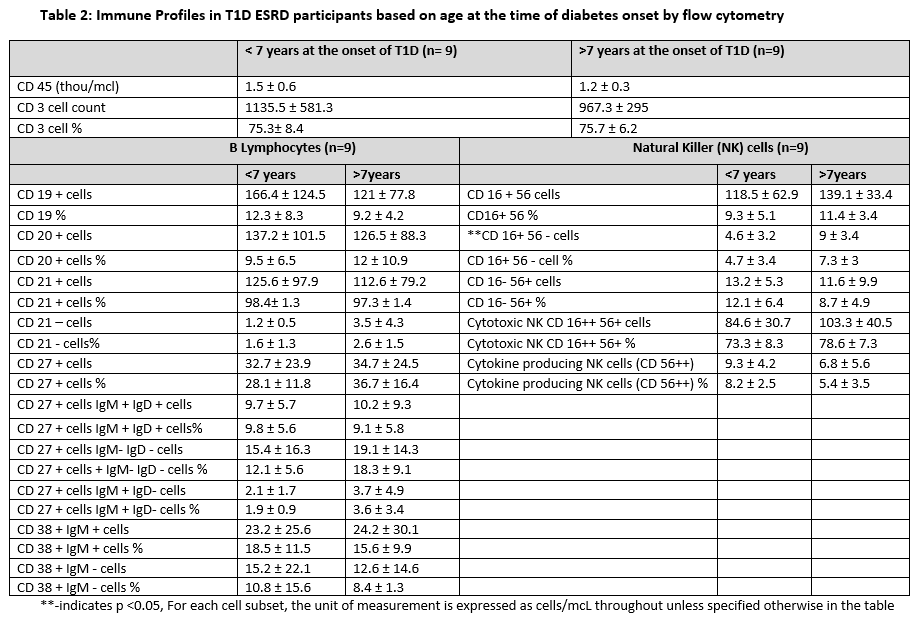
Methods: After IRB approval, we prospectively performed quantitative B cell and Natural Killer (NK) cell subset immunophenotyping by flow cytometry, and measured Immunoglobulin (IgA, IgM and IgG) levels by Nephelometry on 18 T1D subjects with ESRD waitlisted for Simultaneous Pancreas and Kidney Transplantation (SPK) in two age and gender matched groups of patients: a) onset < 7 yrs. (Group 1, n=9), and b) onset > 7 yrs. (Group 2, n=9).
Results: Detailed baseline demographics of the two groups are shown under Table 1, both groups were comparable. B cells, NK cells and their subsets are shown in Table 2. Group 1 showed a significantly lower number of CD 16+ 56- cells (p-value 0.027) as compared to group 2; other cells count, and percentages were not significantly different.
Conclusion: While previous work has shown a link between altered NK cells and the early onset of type I diabetes, our data do not show a significant difference in the major NK cell subsets between the two groups of patients. Additional studies with a larger sample size could help resolve this disparity.